



초록접수 현황
| 17F-211 | 구연 미채택시 포럼 발표 |
Clinical Outcome and Cost Analysis of Rapid Deployment Aortic Valve Replacement Versus Transcatheter Aortic Valve Implantation: A Single Center Early Experience
Mi Hee Lim, Hyung Gon Je, Sang-Kwon Lee, Ji Hye Lee, Hye Rim Oh
Department of Cardiovascular and Thoracic Surgery, Pusan National University Yangsan Hospital, Pusan National University College of Medicine, Gyeongsangnam-do, Republic of Korea
Purpose : Surgical rapid deployment and interventional transcatheter aortic valve replacement have been adopted since October 2015 in our hospital. An initial analysis was carried out to compare the early clinical outcome and costs of these approaches.
Methods : Between October 2015 and July 2017, 17 patients underwent rapid deployment aortic valve replacement with the Intuity valve (group RDAVR) and 11 patients implanted Evolute-R as a transcatheter aortic valve implantation (group TAVI).
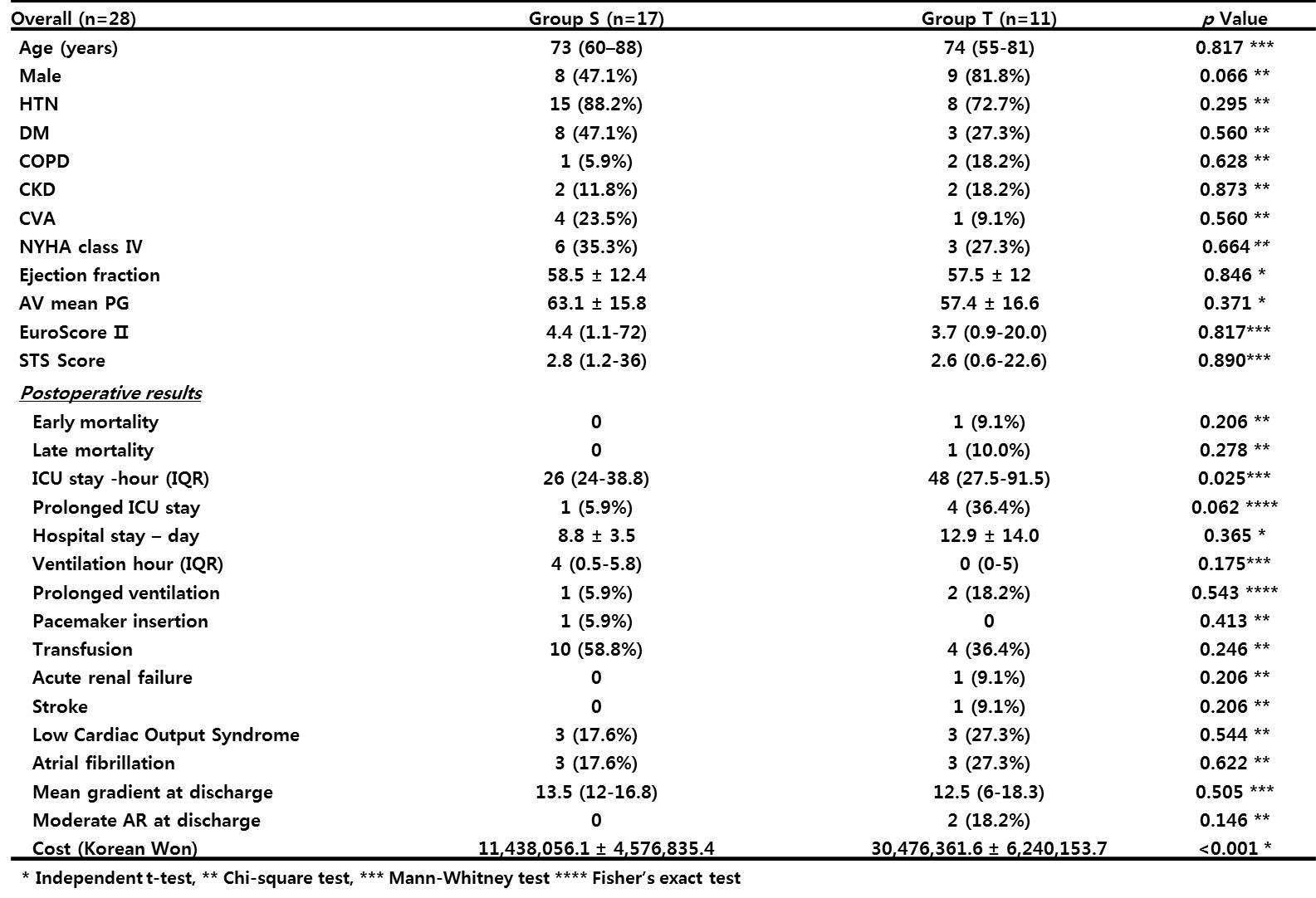
Results : Patients of both groups showed similar characteristics including age, gender, hypertension, diabetes, NYHA class 4. The estimated surgical mortality, which calculated by EuroSCORE II (RDAVR: 4.4 (1.1-72) vs TAVI: 3.7 (0.9-20); p=0.817) and STS score (RDAVR: 2.8 (1.2-36) vs. TAVI: 2.6 (0.6-22.6; p=0.890) was comparable between groups. Only 1 hospital mortality developed in TAVI group. The incidence of major complication such as permanent pacemaker insertion, acute renal failure, stroke, prolong ventilation were comparable between groups but ICU stay was significantly longer in TAVI group. Mean gradients were equivalent at discharge (RDAVR: 13.5 (12-16.8) vs. TAVI: 12.5 (6-18.3) mmHg, p = 0.505). At discharge 2 patients in TAVI group had 3+ aortic insufficiencies (AI) which were closely observed without further intervention. One patient in RDAVR group showed 1+ AI which progress to 3+ and underwent reoperation. The cost paid by the patient was almost triple for TAVI patients. (Table)
Conclusion : The early clinical results of surgical aortic valve replacement with the Intuity system are comparable to TAVI in our early experience. On the aspect of patient paying cost, TAVI is more expensive than RDAVR.
Methods : Between October 2015 and July 2017, 17 patients underwent rapid deployment aortic valve replacement with the Intuity valve (group RDAVR) and 11 patients implanted Evolute-R as a transcatheter aortic valve implantation (group TAVI).
Results : Patients of both groups showed similar characteristics including age, gender, hypertension, diabetes, NYHA class 4. The estimated surgical mortality, which calculated by EuroSCORE II (RDAVR: 4.4 (1.1-72) vs TAVI: 3.7 (0.9-20); p=0.817) and STS score (RDAVR: 2.8 (1.2-36) vs. TAVI: 2.6 (0.6-22.6; p=0.890) was comparable between groups. Only 1 hospital mortality developed in TAVI group. The incidence of major complication such as permanent pacemaker insertion, acute renal failure, stroke, prolong ventilation were comparable between groups but ICU stay was significantly longer in TAVI group. Mean gradients were equivalent at discharge (RDAVR: 13.5 (12-16.8) vs. TAVI: 12.5 (6-18.3) mmHg, p = 0.505). At discharge 2 patients in TAVI group had 3+ aortic insufficiencies (AI) which were closely observed without further intervention. One patient in RDAVR group showed 1+ AI which progress to 3+ and underwent reoperation. The cost paid by the patient was almost triple for TAVI patients. (Table)
Conclusion : The early clinical results of surgical aortic valve replacement with the Intuity system are comparable to TAVI in our early experience. On the aspect of patient paying cost, TAVI is more expensive than RDAVR.
책임저자: Hyung Gon Je
Department of Cardiovascular and Thoracic Surgery, Pusan National University Yangsan Hospital, Pusan National University College of Medicine, Gyeongsangnam-do, Republic of Korea
발표자: Mi Hee Lim, E-mail : jehg7332@gmail.com